| Name | Estradiol |
| Classes |
Dermatological/Topical Agent Hormonal Agent Sex Hormone Steroid Vaginal Preparation |
| Diseases |
Dryness Genito-Urinary Disease Itching Menopause |
 Bangla
Bangla English
EnglishEstradiol
Estradiol is an estrogen hormone and the major female sex hormone. Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Through a negative feedback mechanism, circulating estrogens modulate pituitary secretion of gonadotropins such as luteinizing hormone (LH) and follicle stimulating hormone (FSH). Estrogens work to reduce postmenopausal women's elevated levels of these hormones.
Estradiol is indicated in the:
- Treatment of moderate to severe vasomotor symptoms associated with the menopause.
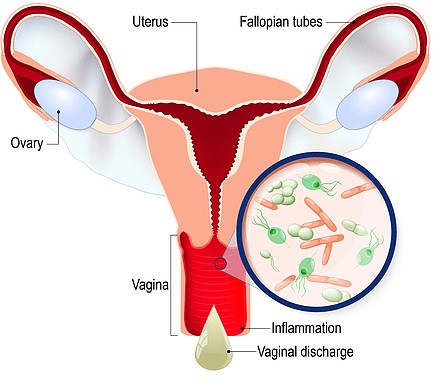
- Treatment of moderate to severe symptoms of vulvar and vaginal atrophy associated with the menopause. When prescribing solely for the treatment of symptoms of vulvar and vaginal atrophy, topical vaginal products should be considered.
- Treatment of hypoestrogenism due to hypogonadism, castration or primary ovarian failure.
- Treatment of breast cancer (for palliation only) in appropriately selected women and men with metastatic disease.
- Treatment of advanced androgen-dependent carcinoma of the prostate (for palliation only).
- Prevention of osteoporosis.

- Vasomotor symptoms associated with the menopause: The usual initial dosage range is 1 to 2 mg daily of estradiol adjusted as necessary to control presenting symptoms. The minimal effective dose for maintenance therapy should be determined by titration. Administration should be cyclic (e.g., 3 weeks on and 1 week off).
- Female hypoestrogenism: Treatment is usually started with a dose of 1 to 2 mg of estradiol daily, which is then adjusted as needed to control the presenting symptoms; the minimal effective dose for maintenance therapy should be determined through titration.
- Breast cancer (for palliation only): Suggested dosage is 10 mg three times daily for a period of at least three months.
- Advanced androgen-dependent carcinoma of the prostate (palliation only): The recommended dosage is 1 to 2 mg three times per day. The effectiveness of therapy can be determined by phosphatase determinations as well as the patient's symptomatic improvement.
- Prevention of osteoporosis: When prescribing solely for the prevention of postmenopausal osteoporosis, therapy should be considered only for women who are at high risk of osteoporosis and who are not candidates for non-estrogen medications.
- Genitourinary system: Changes in vaginal bleeding pattern and abnormal withdrawal bleeding or flow; breakthrough bleeding, spotting, dysmenorrhea Increase in size of uterine leiomyomata, Vaginitis, including vaginal candidiasis, Change in amount of cervical secretion, Changes in cervical ectropion, Ovarian cancer; endometrial hyperplasia; endometrial cancer.
- Breasts: Tenderness, enlargement, pain, nipple discharge, galactorrhea; fibrocystic breast changes; breast cancer.
- Cardiovascular: Deep and superficial venous thrombosis; pulmonary embolism; thrombophlebitis; myocardial infarction; stroke; increase in blood pressure.
- Gastrointestinal: Nausea, vomiting, Abdominal cramps, bloating, Cholestatic jaundice, Increased incidence of gallbladder disease, Pancreatitis, Enlargement of hepatic hemangiomas.
- Skin: Chloasma or melasma that may persist when drug is discontinued, Erythema multiforme, Erythema nodosum, Hemorrhagic eruption, Loss of scalp hair, Hirsutism, Pruritus, rash.
- Eyes: Retinal vascular thrombosis, Steepening of corneal curvature.
- Central Nervous System: Headache, migraine, dizziness Mental depression, Chorea Nervousness, mood disturbances, irritability, Exacerbation of epilepsy, Dementia.
- Miscellaneous: Increase or decrease in weight, Reduced carbohydrate tolerance, Aggravation of porphyria, Edema Arthralgias, leg cramps, Changes in libido, Urticaria, Angioedema, Anaphylactoid/anaphylactic reactions, Hypocalcemia, Exacerbation of asthma, Increased triglyceride.




ESTROGENS INCREASE THE RISK OF ENDOMETRIAL CANCER
All estrogen-taking women must be closely monitored clinically. In all cases of undiagnosed persistent or recurring abnormal vaginal bleeding, adequate diagnostic measures, including endometrial sampling when indicated, should be taken to rule out malignancy. There is no evidence that using "natural" estrogens at equivalent estrogen doses results in a different endometrial risk profile than using "synthetic" estrogens.
- CARDIOVASCULAR AND OTHER RISKS: Estrogens, whether with or without progestins, should not be used to prevent cardiovascular disease. The Women's Health Initiative (WHI) study found that taking oral conjugated estrogens (CE 0.625 mg) combined with medroxyprogesterone acetate (MPA 2.5 mg) for 5 years increased the risk of myocardial infarction, stroke, invasive breast cancer, pulmonary emboli, and deep vein thrombosis compared to placebo.
- Venous thromboembolism (VTE): In the Women’s Health Initiative (WHI) study, an increase in VTE has been observed in women receiving CE compared to placebo. These observations are preliminary, and the study is continuing.
- Endometrial cancer: The use of unopposed estrogens in women with intact uteri has been associated with an increased risk of endometrial cancer. The reported endometrial cancer risk among unopposed estrogen users is about 2- to 12- fold greater than in non-users, and appears dependent on duration of treatment and on estrogen dose.
- Breast cancer: The use of estrogens and progestins by postmenopausal women has been reported to increase the risk of breast cancer.
- Gallbladder disease: A 2- to 4-fold increase in the risk of gallbladder disease requiring surgery in postmenopausal women receiving estrogens has been reported.
- Hypercalcemia: Estrogen administration may lead to severe hypercalcemia in patients with breast cancer and bone metastases. If hypercalcemia occurs, use of the drug should be stopped and appropriate measures taken to reduce the serum calcium level.
- Visual abnormalities: Retinal vascular thrombosis has been reported in patients receiving estrogens. Discontinue medication pending examination if there is sudden partial or complete loss of vision, or a sudden onset of proptosis, diplopia or migraine. If examination reveals papilledema or retinal vascular lesions, estrogens should be permanently discontinued.
Contraindication
Estradiol is contraindicated in patients hypersensitive to estradiol or any component of the formulation.
None known.
Estrogen is contraindicated in-
- Undiagnosed abnormal genital bleeding.
- Known, suspected or history of cancer of the breast except in appropriately selected patients being treated for metastatic disease.
- Known or suspected estrogen-dependent neoplasia.
- Active deep vein thrombosis, pulmonary embolism or history of these conditions.
- Active or recent (e.g., within the past year) arterial thromboembolic disease (e.g., stroke, myocardial infarction).
- Liver dysfunction or disease.
- Known or suspected pregnancy.